Authored by:
Bill Johnson DNAP, CRNA
Director, Acute Surgical Pain Management Fellowship and Doctorate Completion Program Middle Tennessee School of Anesthesia

Overview
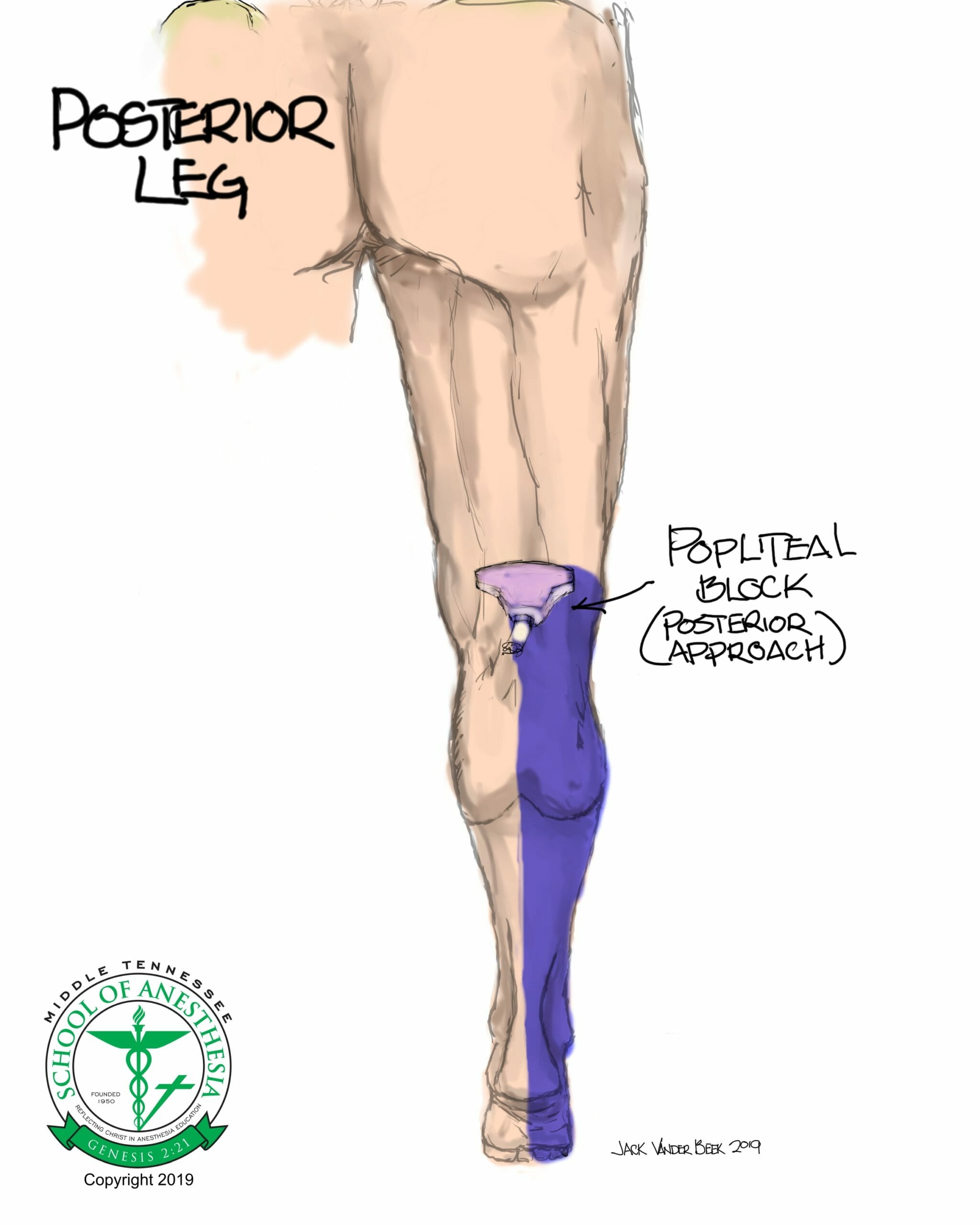
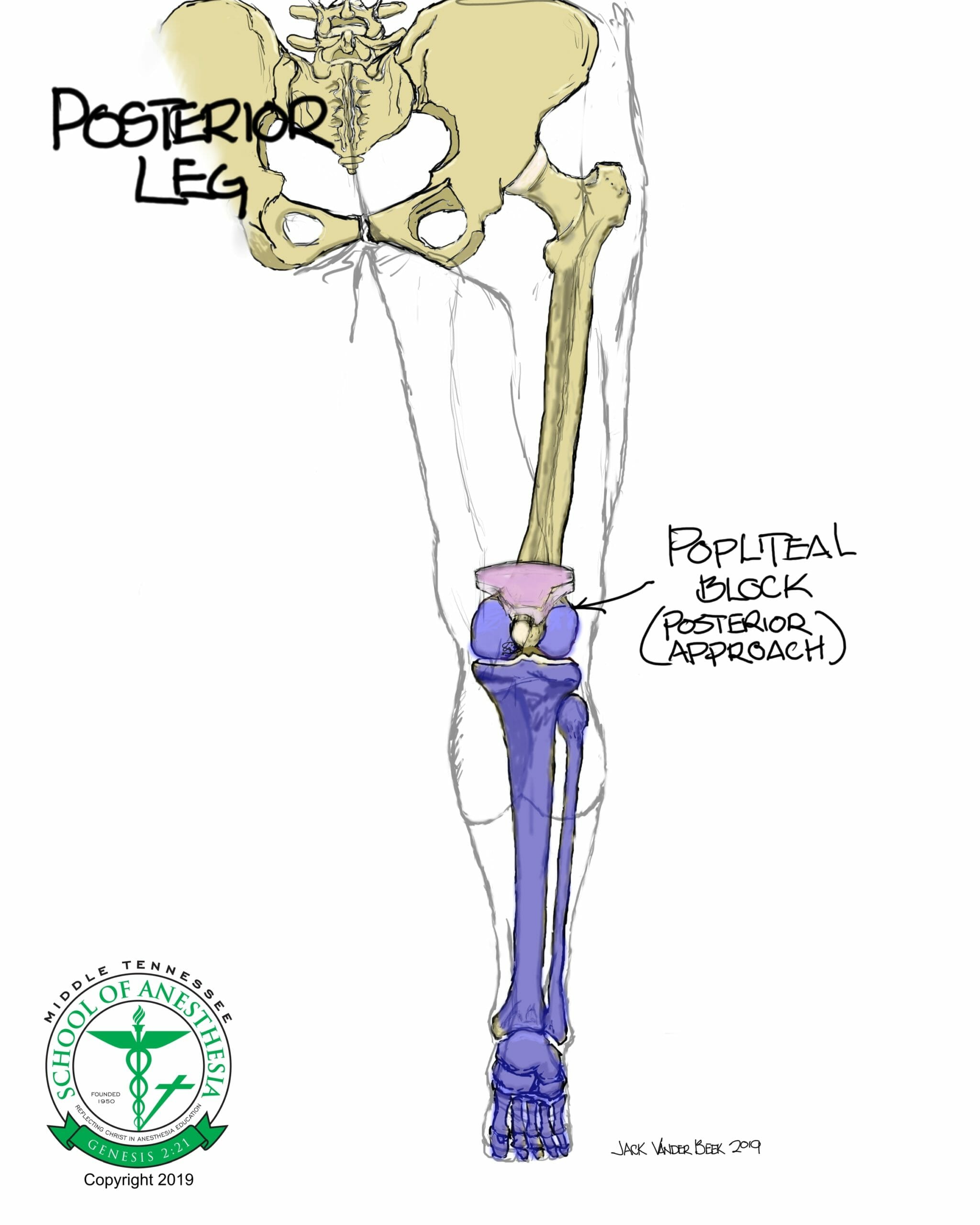
- A block of the distal sciatic nerve provides surgical coverage for surgeries involving the posterolateral calf and foot regions with the exception of the medial ankle which is innervated primarily by the saphenous nerve.
- Blockade of the sciatic nerve will result in diminished plantar and dorsal flexion strength of the foot and impair postoperative ambulation.
Indications
Any surgery involving the posterior calf, ankle (no medial coverage), and foot.
Positioning
Block can be performed in the supine, prone, or lateral position depending on patient’s body habitus, pain level with positioning, and regionalist’s skill level in performing the block.
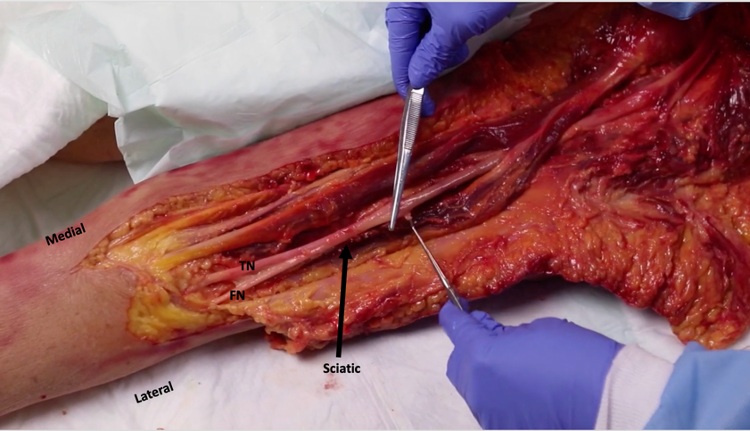
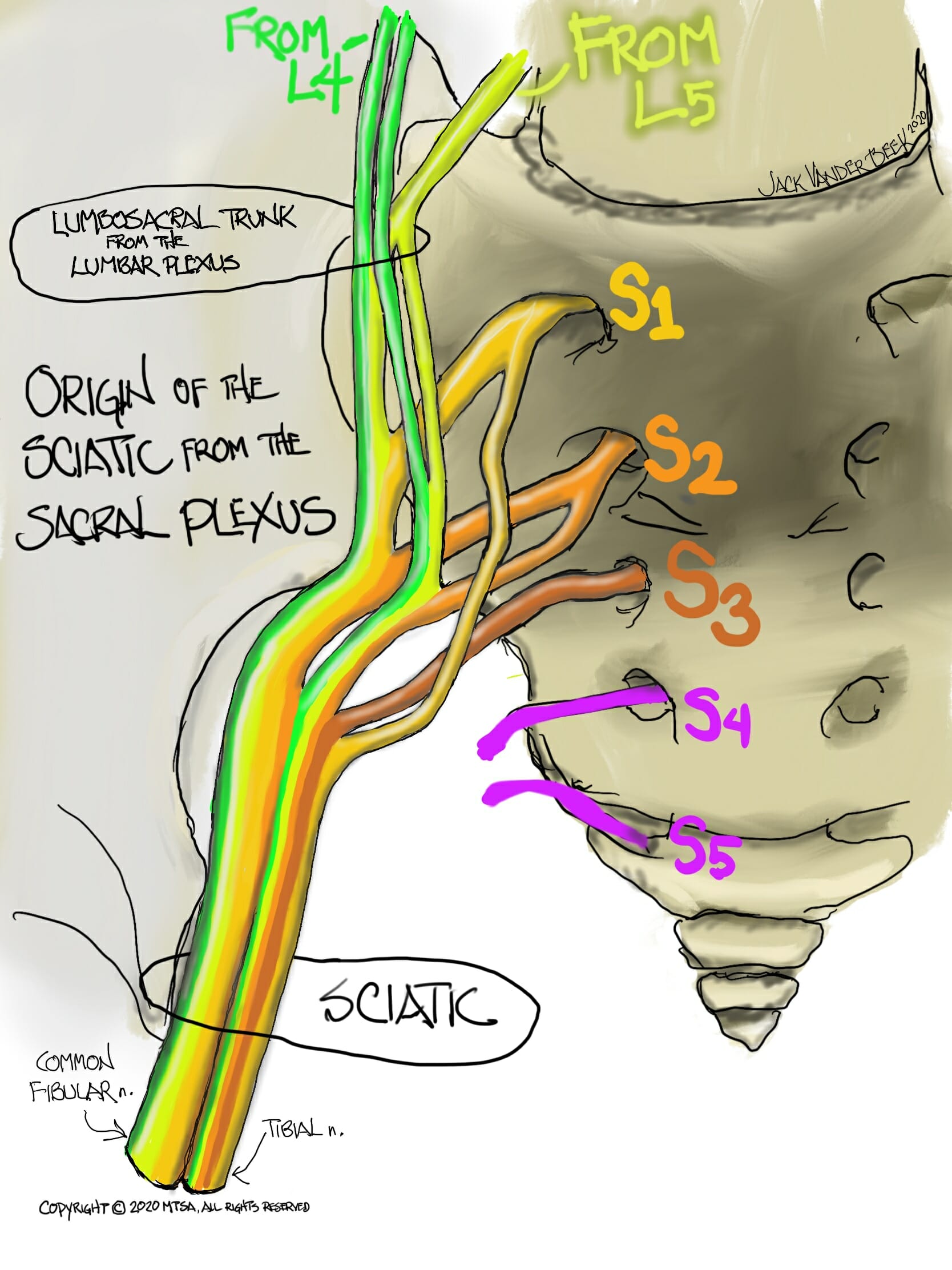
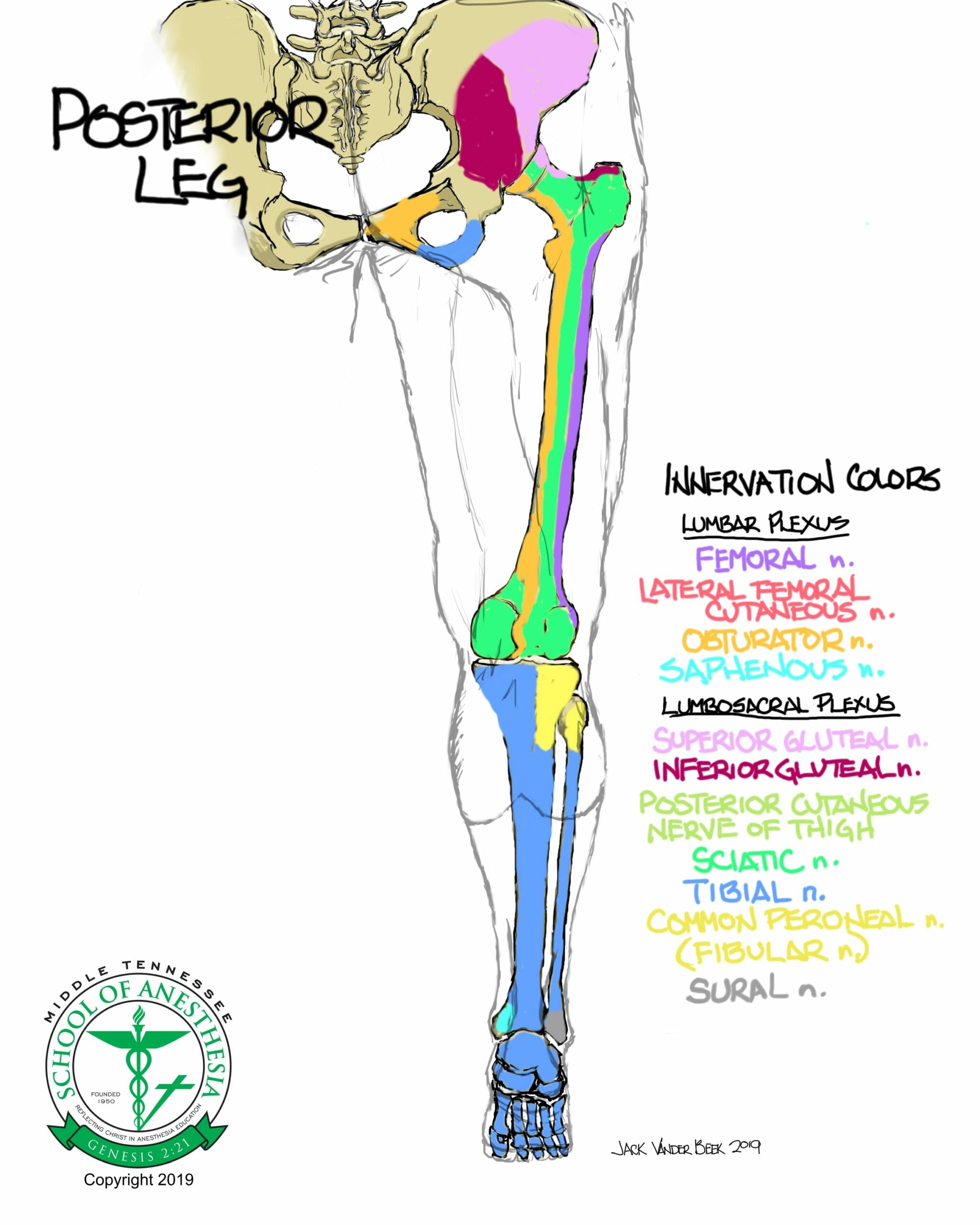
Anatomy of the Distal Sciatic (Popliteal) Nerve
- The sciatic nerve originates from the L4-L5 and S1-S3 ventral rami roots of the spinal cord.
- From the level of the lumbosacral plexus, the sciatic nerve is comprised of two primary peripheral nerves (fibular/peroneal and tibial) which are isolated and contained within two separate neural sheaths until they bifurcate and separate away from each other, 6-8 cm proximal to the popliteal crease. Bifurcation and separation of the fibular and tibial nerves can occur at a more proximal thigh location in certain individuals.
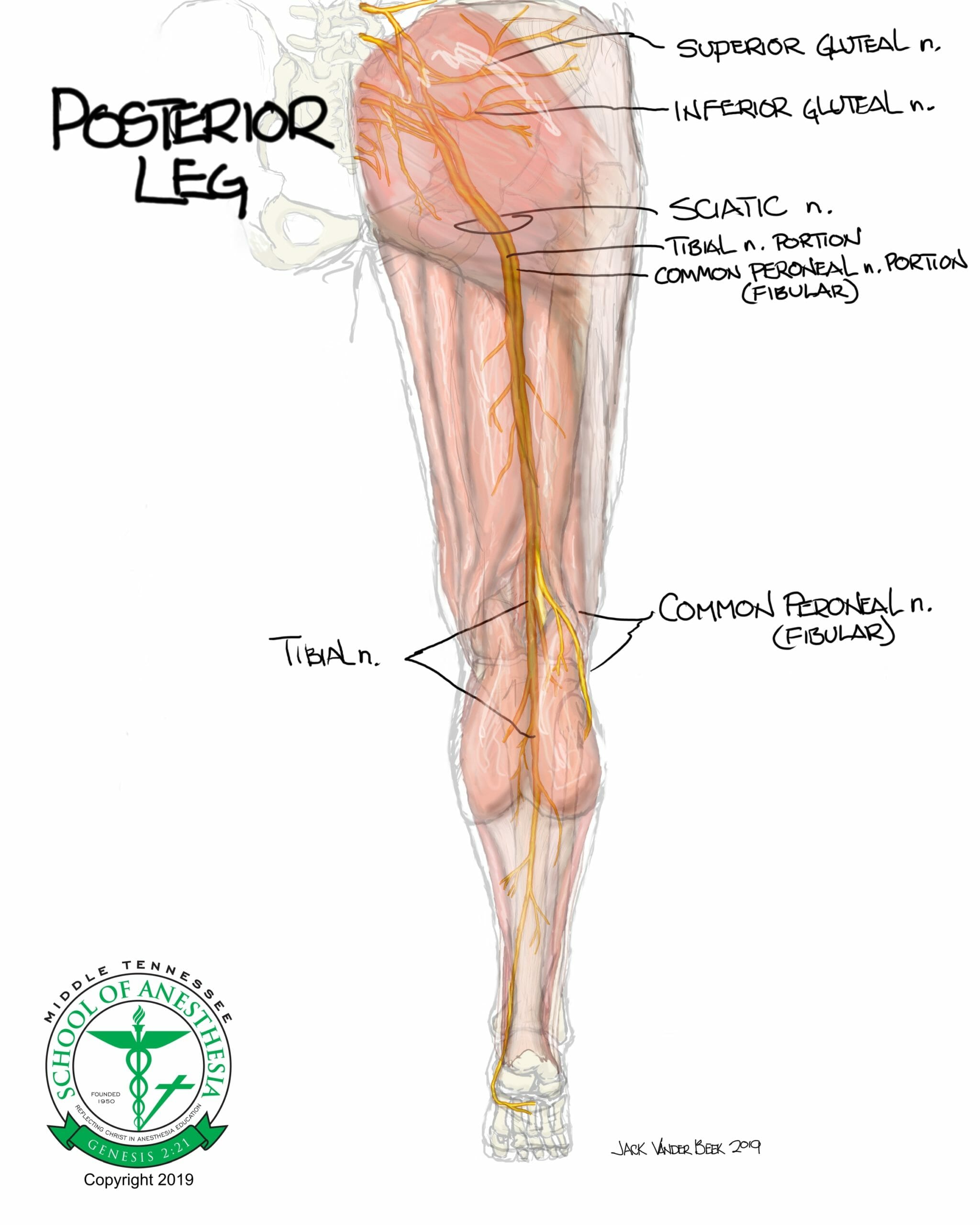
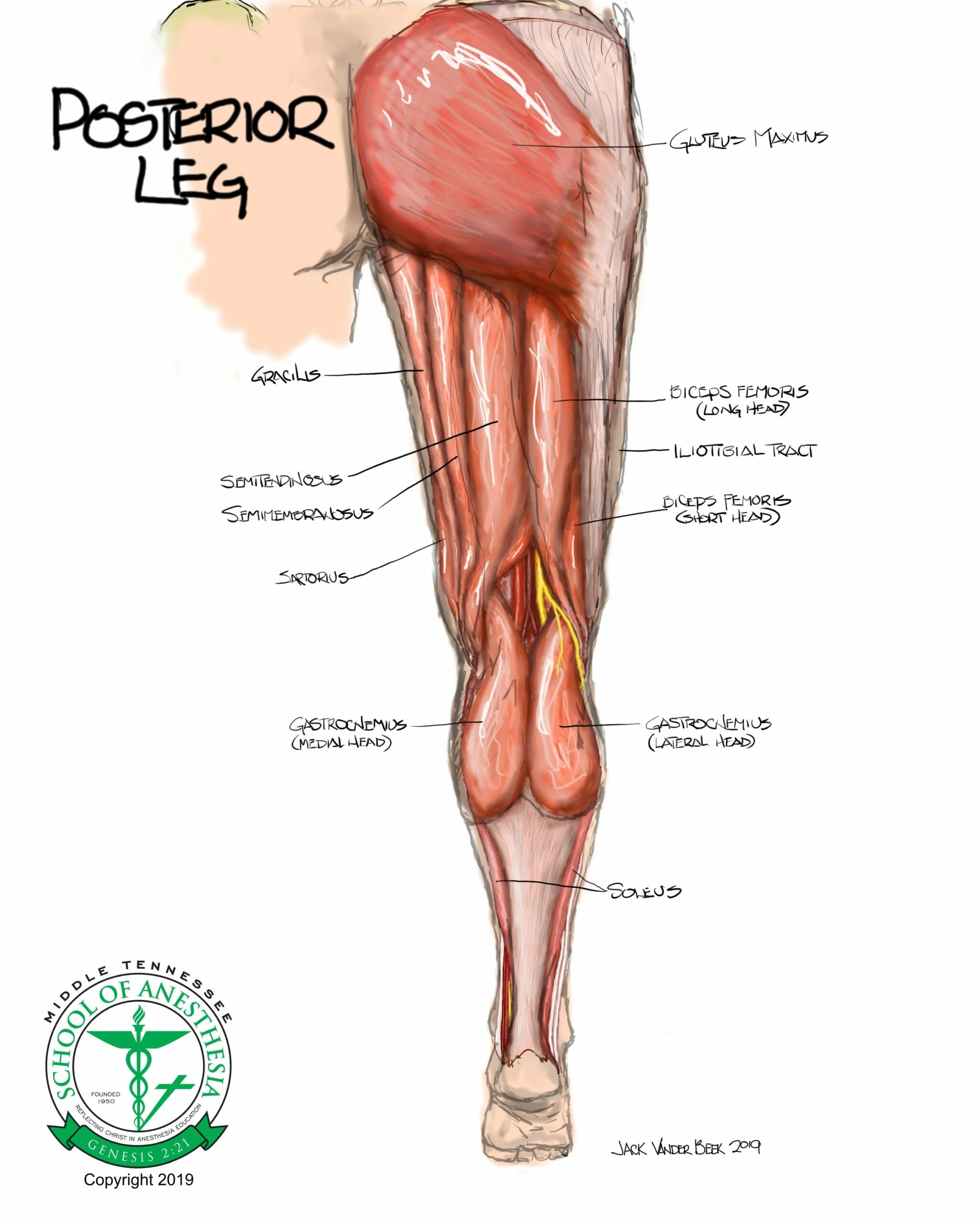
- The sciatic nerve is derived from the lumbosacral plexus and descends into the pelvis through the greater sciatic foramen and exits inferior to the piriformis muscle to supply sensory and motor innervation to the gluteal region and posterior aspects of the thigh that lie deep to the rectus femoris muscle.
- Motor branches from the sciatic nerve supply the semimembranosus, semitendinosus, biceps femoris, and adductor longus muscles.
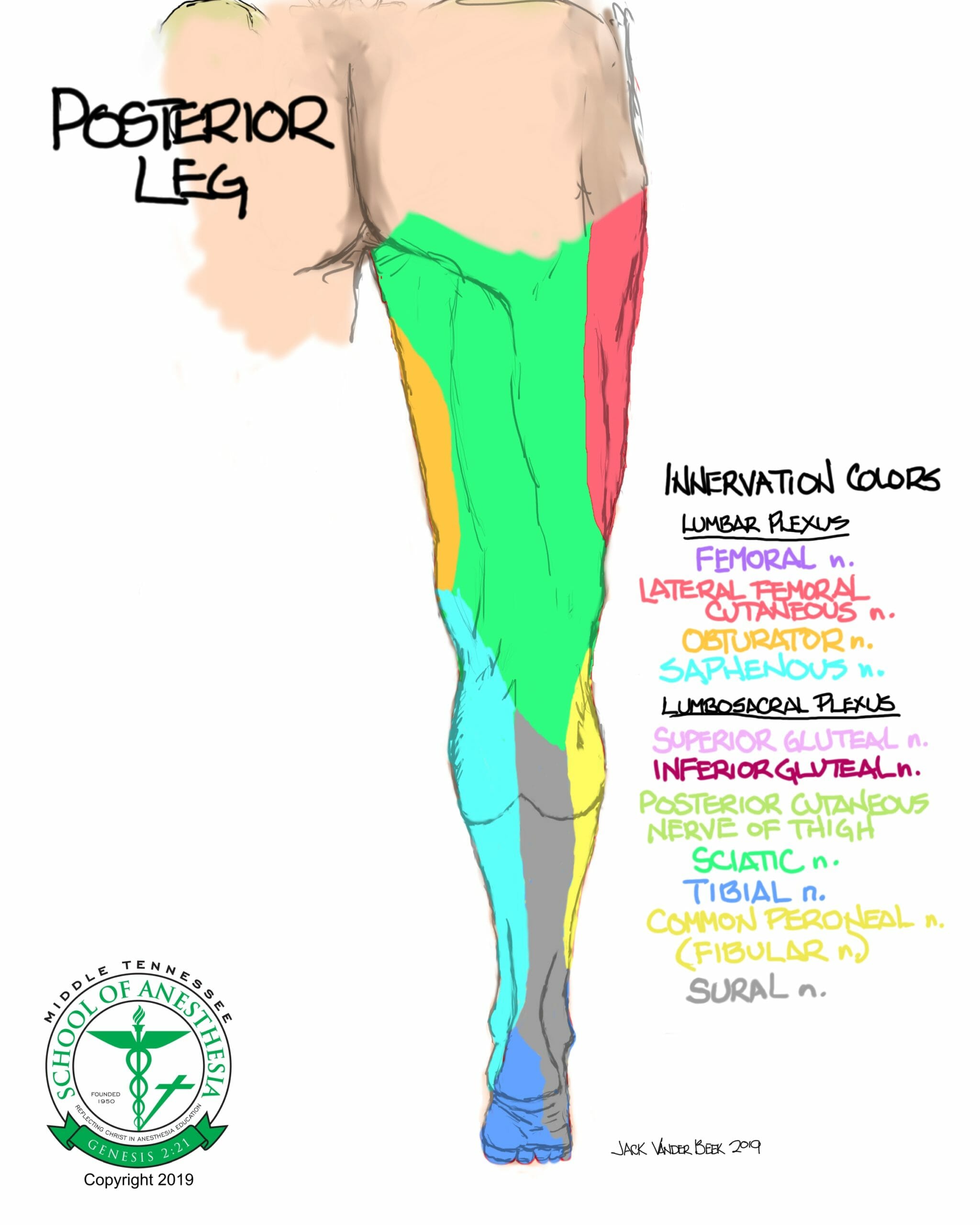
Dermatome Coverage
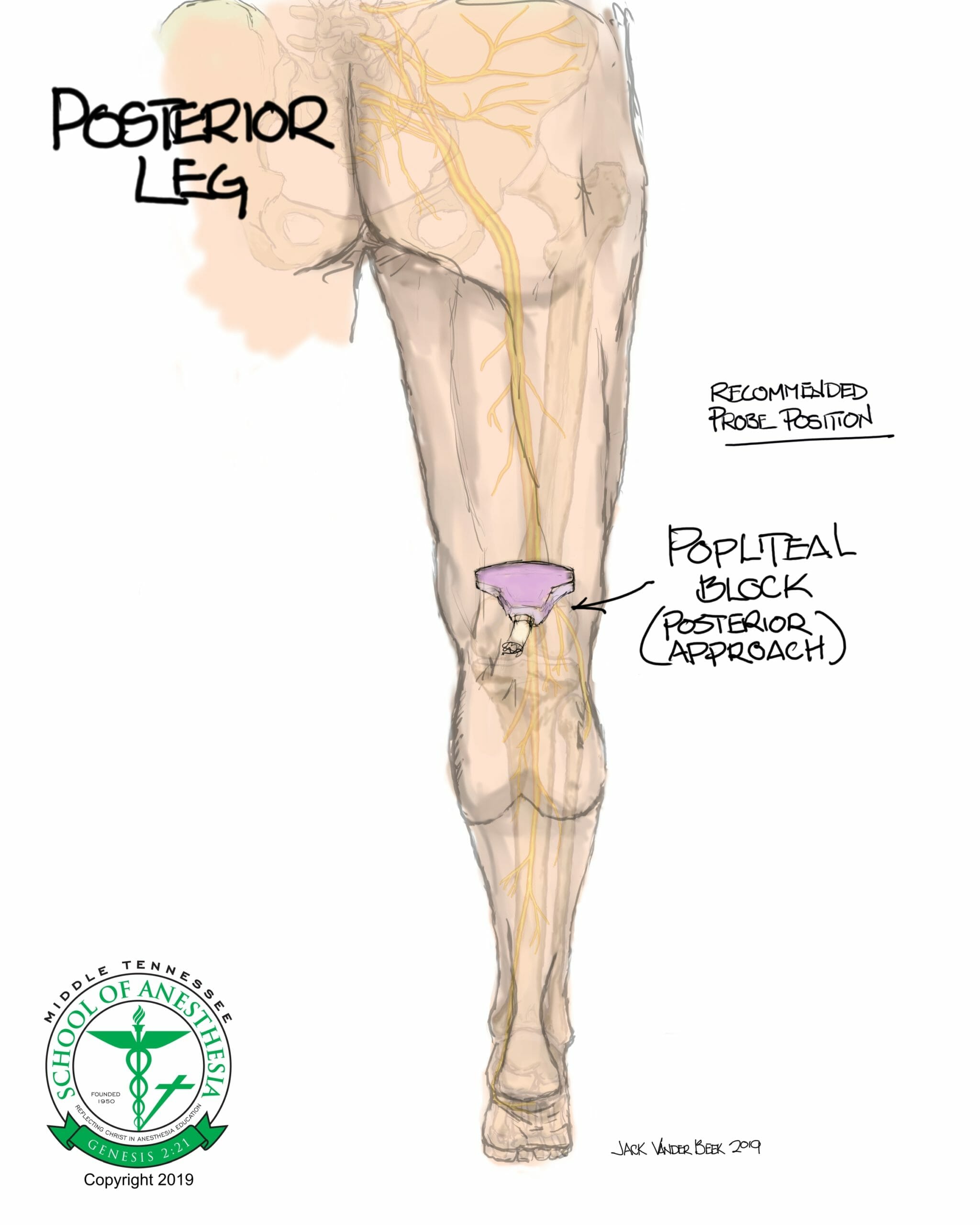
Surface Landmarks
Common probe placement for the distal sciatic nerve block is 6-8 cm proximal to the popliteal crease with the probe placed in a slightly lateral position on the leg. (See scanning techniques).
Scanning Technique
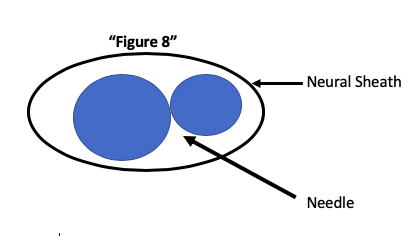
Begin scanning in the popliteal crease area and locate the popliteal artery and vein. Superior to these vasculature structures, the tibial nerve often can be visualized be tilting the probe until a hyperechoic structure is seen on ultrasound. From this location in the popliteal crease, move the probe proximally until the unification of the tibia and fibular (peroneal) are discovered and represented as a hyperechoic, “Figure 8” on the ultrasound screen.
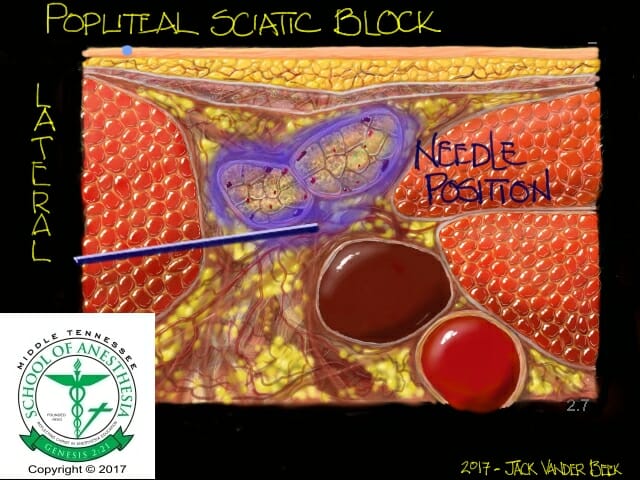
Sonoanatomy
Needle Approach
Lateral

Supine

- A tangential approach should be taken when directing the needle towards the sciatic nerve. The needle tip should enter the sciatic neural sheath at the center of the “Figure 8,” avoiding direct needle-to-nerve contact.
Nerve Stimulator Guidance
- The sciatic nerve is responsible for motor function of the foot that can be remembered using the following acronym: “TIPPED” (Tibial Inversion and Plantarflexion; Peroneal Eversion and Dorsiflexion)
- Advance needle until a motor response twitch is obtained in the 0.3-0.5 mA range. Loss of a twitch response should occur with a stimulator voltage < 0.2 mA to avoid a intraneural injection of local anesthetic.
Injection Techniques
- The need should be directed into the sheath at a location between the tibial and peroneal (fibular) nerve.
- Small aliquot injections of 3-5 ml should be made that will result in slight separation of the nerves. Once there is space generated between the sheath and the nerves, an additional needle attempt placement above the nerves can be performed to circumferentially surround the nerves with local anesthetic.
Local Anesthetic Volume
- Distal Sciatic (Popliteal) Nerve: 20-25 ml
Catheter Techniques
- Catheters can be placed for extended analgesia.
- With the needle angled in a slightly oblique fashion and the Tuohy tip directed towards the foot, a catheter can be threaded 3-5 cm into the distal sciatic sheath utilizing an in-plane or out-of-plane needling approach.
- Distal sciatic catheters can be placed parallel to the sciatic nerve if positioned 3-5 cm proximal to the bifurcation point of the tibial and peroneal/fibular nerve. This method facilitates better local anesthetic distribution, reduces the volume of local anesthetic from leaking from the insertion point, and minimizes catheter migration or displacement.
- Continuous Infusions can started at rate of 4-6 ml/hr.
Complications
- Local anesthetic toxicity (LAST)
- Infection
- Hematoma
- Nerve injury
- Persistent neuropathy
- Ambulation injuries: Patient should be instructed to avoid ambulating until full ankle/foot strength has returned following a regional block.
- Foot drop from persistent fibular/peroneal nerve blockade
PEARLS
- Performing the block in the supine position will result in needle movements that are represented on the ultrasound machine in an inverse fashion. When directing the needle to a superficial location, the needle will be physically directed downward or towards the probe which will appear on the ultrasound screen as the needle moving in an upward fashion.
- Targeted tibial nerve blocks can be performed for posterior knee analgesic coverage for total knee arthroplasty cases. Perform tibial nerve block in a location at least 4-5 cm distal from the bifurcation point of the sciatic nerve, isolate the motor twitch response with a nerve stimulator (inversion and plantarflexion of the foot), and limit local anesthetic volume to 6-8 ml to avoid peroneal/fibular nerve blockade and foot drop from occurring postoperatively.
- Persistent neuropathies with the popliteal block, especially in the diabetic population, have been reported in the literature and can be reduced by minimizing local anesthetic concentrations to analgesic strengths whenever possible, reducing local anesthetic volume utilize in the block, and limiting surgical tourniquet times.
- Avoidance of adjuncts for prolonging block duration in diabetic patients is also warranted.
References
- Hadzic, Admir. Hadzic’s textbook of regional anesthesia and acute pain management. McGraw Hill Professional, 2017.
- Chan V and Pollard B. An Introductory Curriculum for Ultrasound-Guided Regional Anesthesia; Univeristy of Toronto Press, 2009.
- Gray, A. Atlas of Ultrasound-Guided Regional Anesthesia. Suanders/Elsevier, 2007.
- Monahan AM, Madison SJ, Loland VJ, Sztain JF, et al. Continuous popliteal sciatic nerve blocks: Does varying perineural catheter location relative to the sciatic bifurcation influence block effects? A dual-center, randomized, subject-masked, controlled clinical trial. Anesth Analg. 2016;122(5):1689-1695.
- Anderson JG, Bohay DR, Maskill JD, Gadkari KP, et al. Complications after popliteal block for foot and ankle surgery. Amer Ortho Foot & Ankle Surg. 2015;36(10):1138-1143.