Authored by:
Bill Johnson DNAP, CRNA
Director, Acute Surgical Pain Management Fellowship and Doctorate Completion Program Middle Tennessee School of Anesthesia

Overview
- A block of the femoral nerve provides surgical or analgesic coverage for surgeries of the anteromedial aspect of the lower extremity.
- Blockade of the femoral nerve will result in quadricep weakness and limited weight-bearing activites of the affected extremity.
Indications
Surgical indications include: Total knee arthroplasty, ACL/MCL knee repairs, patella fractures, or any surgery involving the anteromedial aspects of the lower extremity.
Positioning
Supine
Anatomy of the Femoral Nerve
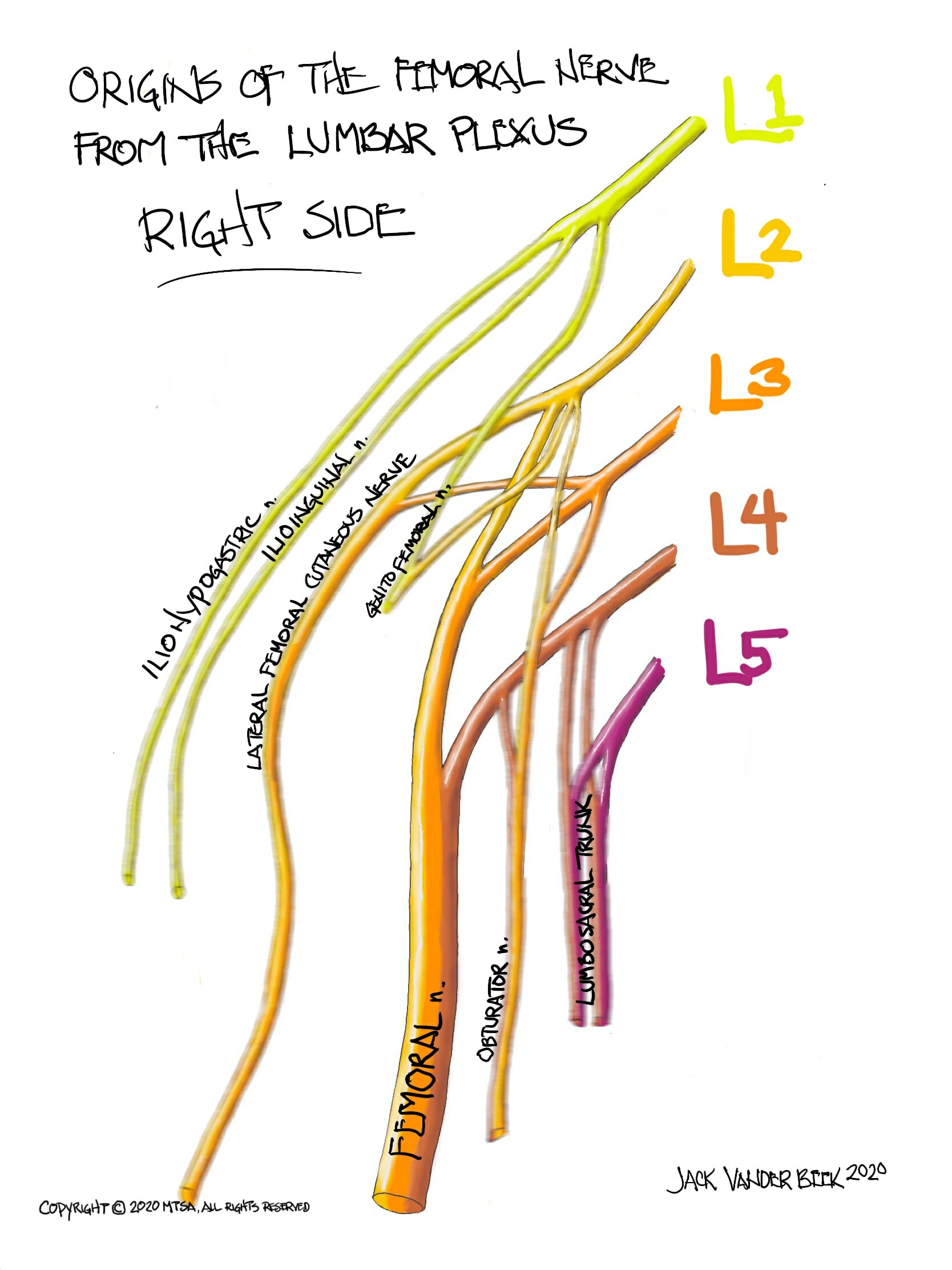
- The femoral nerve originates from the L2-L4 ventral rami roots and is the largest terminal nerve of the lumbar plexus.
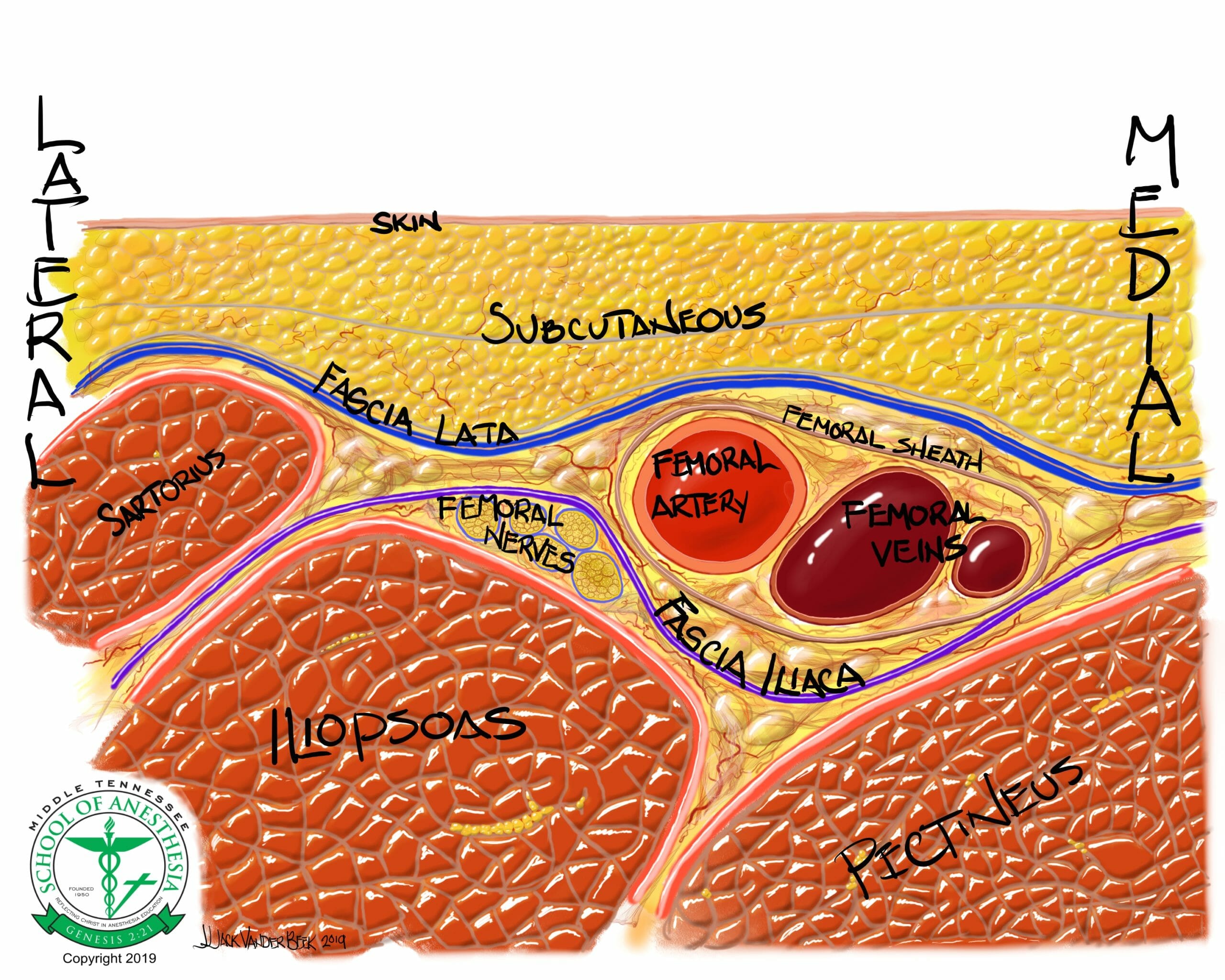
- The femoral nerve courses between the psoas major and quadratus lumborum in the abdominal cavity as it descends and travels distally beneath the inguinal ligament and fascia lata/iliacus layers to innervate the anteromedial aspects of lower extremity (sensory) and provide innervation to quadriceps muscles (motor).
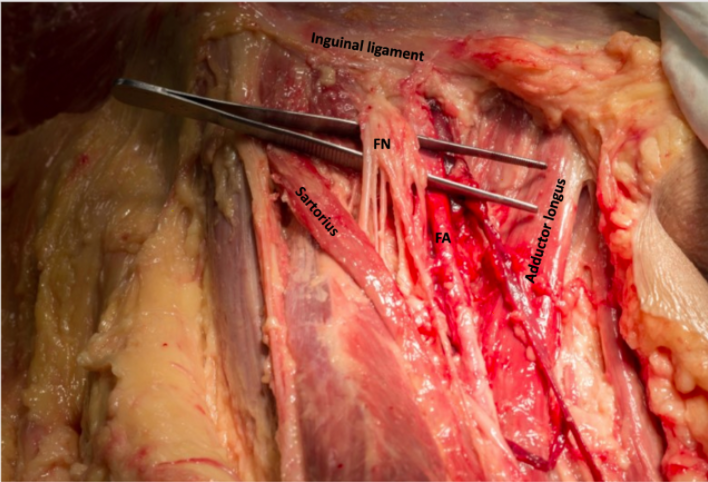
- Below the inguinal ligament, the femoral nerve is located within the “femoral triangle,” which is comprised of anatomic borders comprised of the adductor longus (medial) and sartorius (lateral) muscles.
- The femoral nerve is superficial (2-3 cm below the skin) and is at lateral location to the femoral artery and vein.
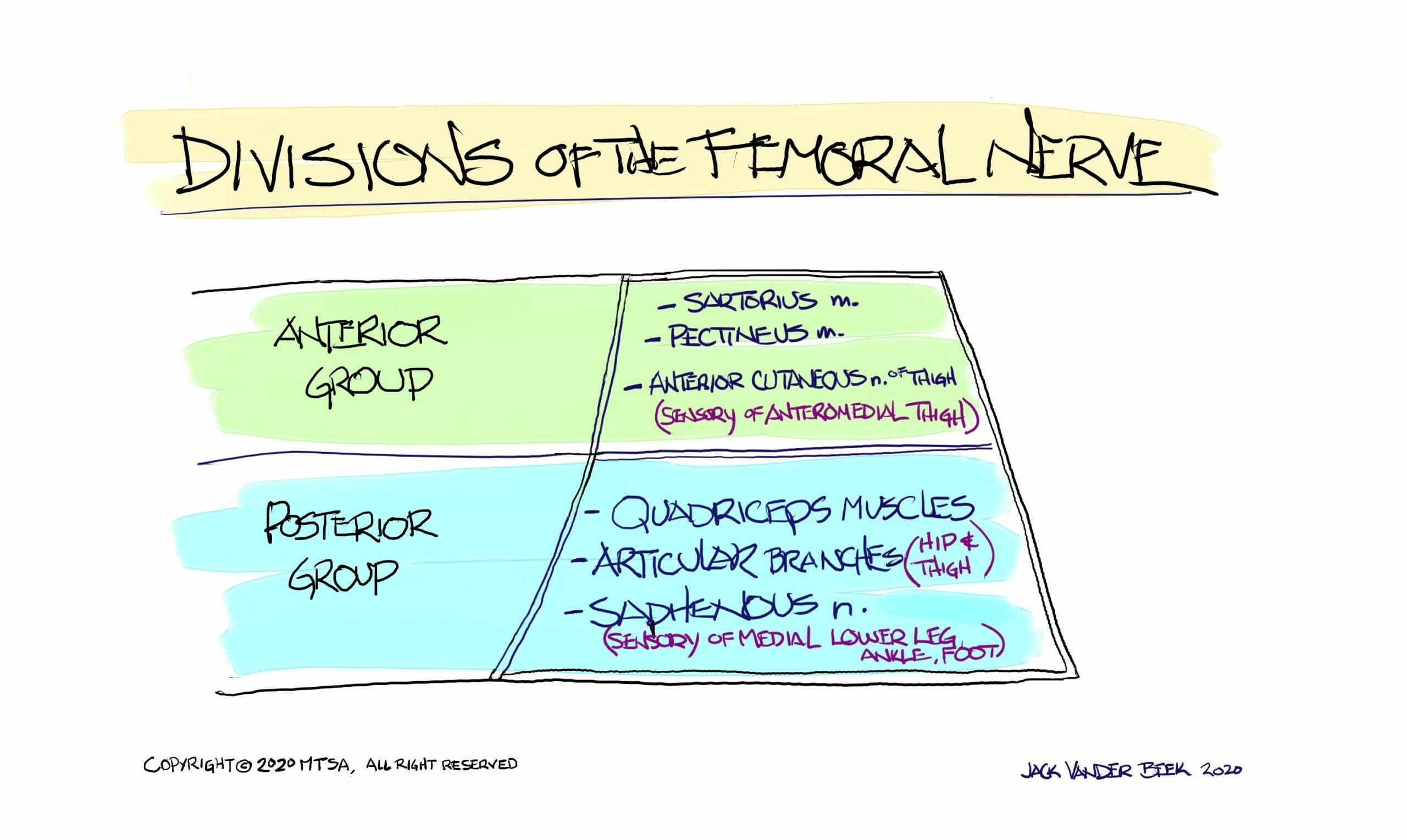
- Within the femoral triangle, the femoral nerve separates into anterior and posterior divisions:
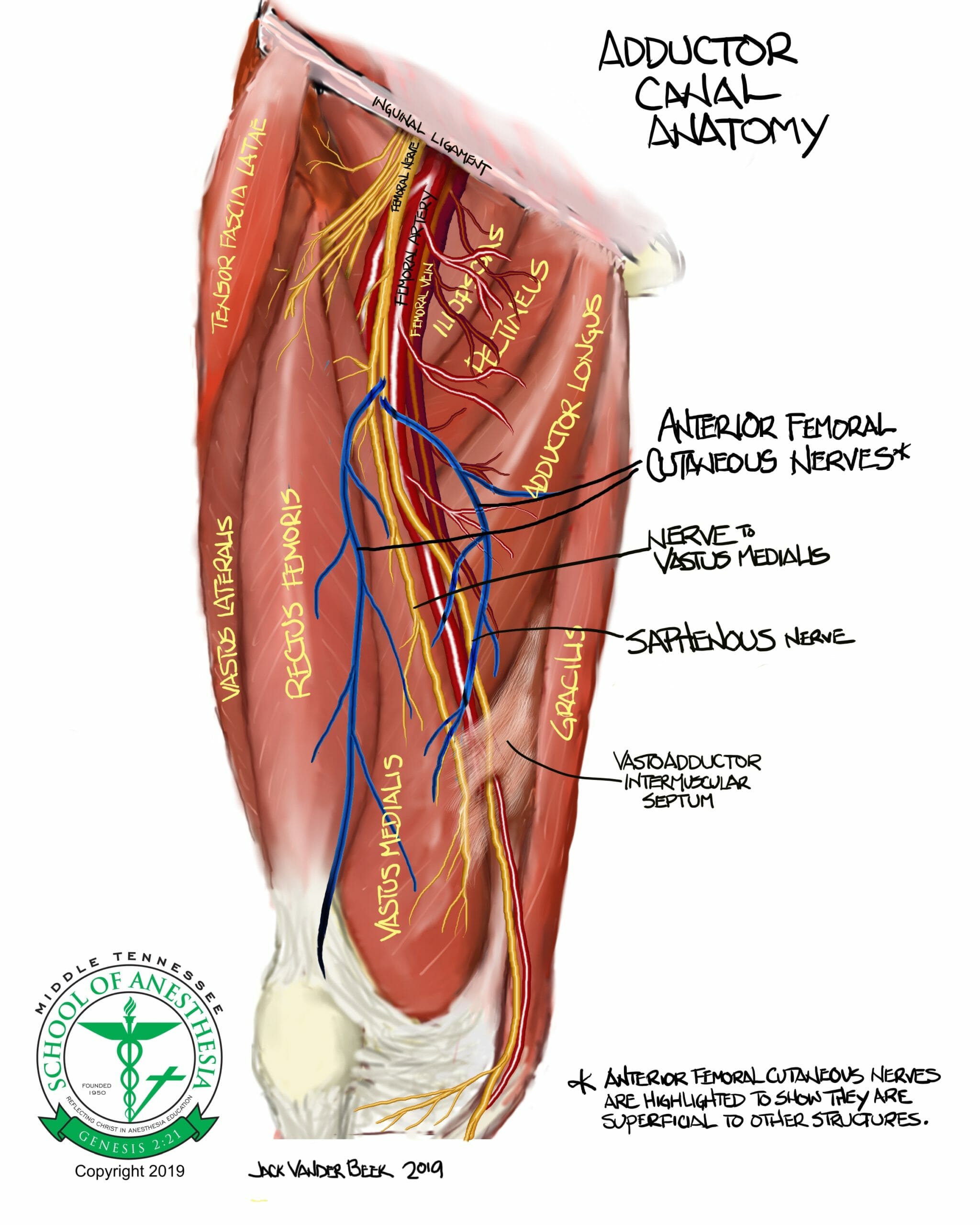
- Anterior division innervates the sartorius and pectineus muscles while giving rise to anterior cutaneous branches that innervate sensory structures of the anteromedial thigh.
- Posterior division innervates the quadricep muscles and the articular branches of the hip and knees. This is also the division that gives rise to the saphenous branch of the femoral nerve.
- The posterior border of the femoral triangle is formed from the iliopsoas (lateral) and pectineus (medial) muscles.
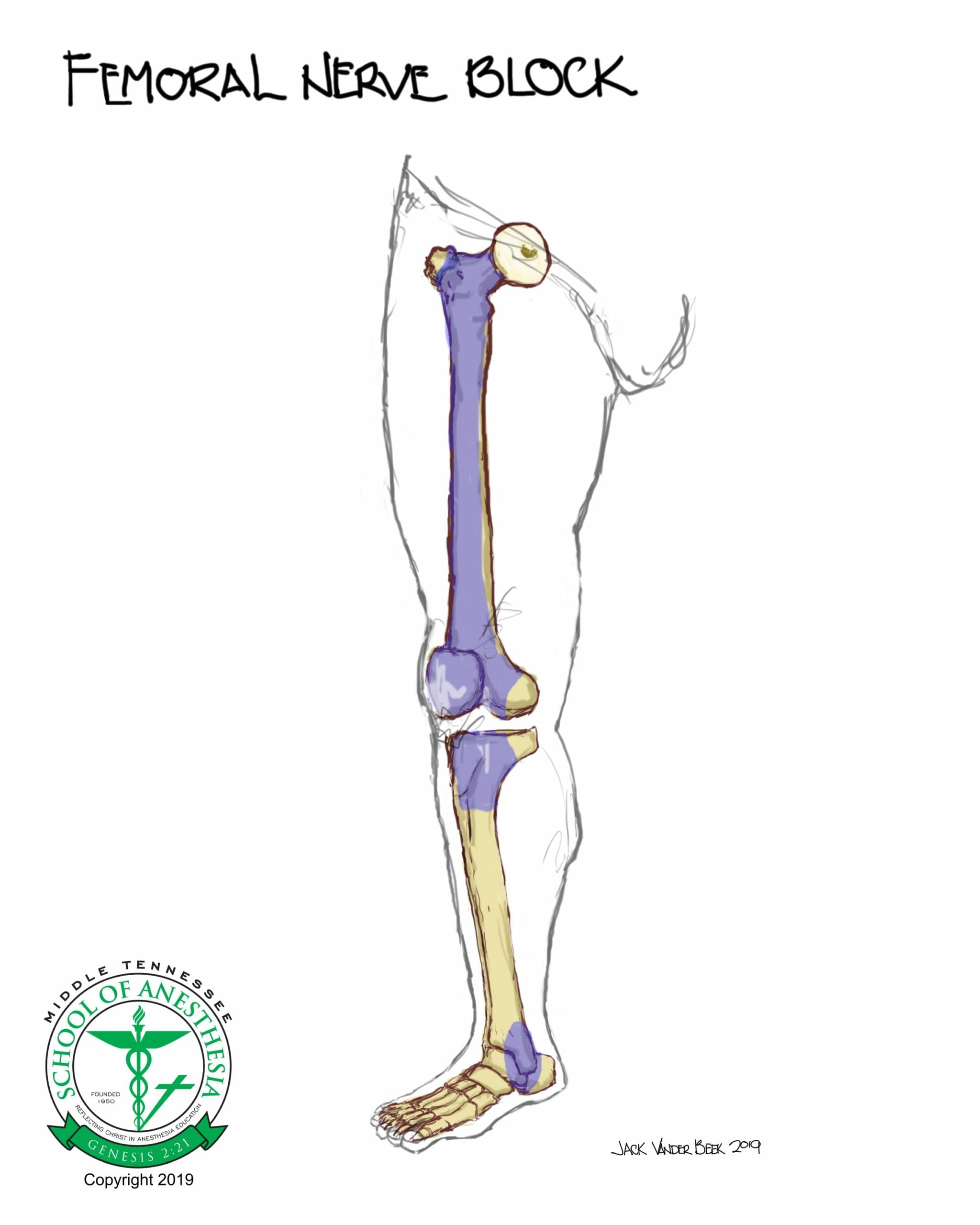
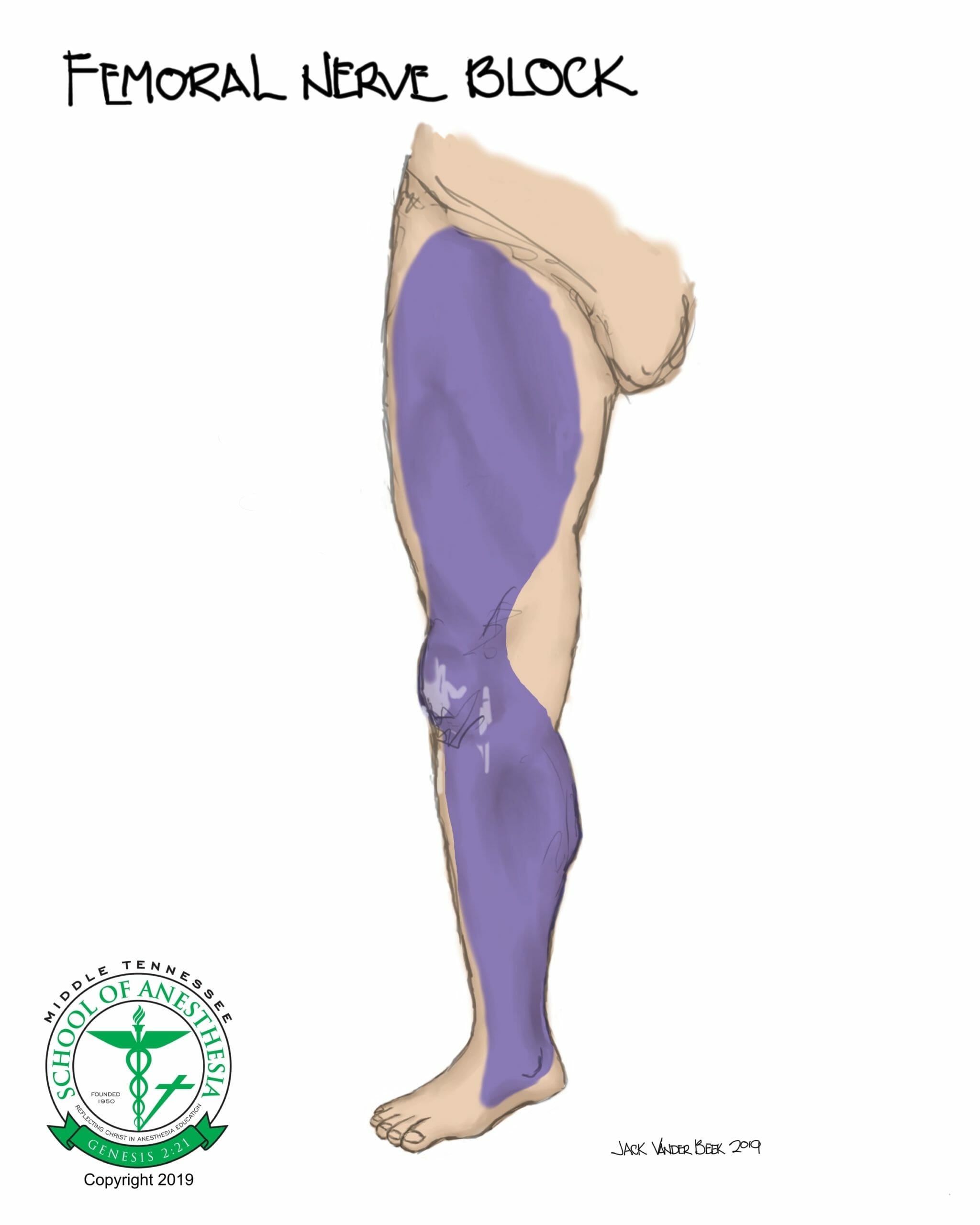
Dermatome Coverage
Dermatome mapping for the femoral nerve and the osteotome distribution are shown in the following illustrations:
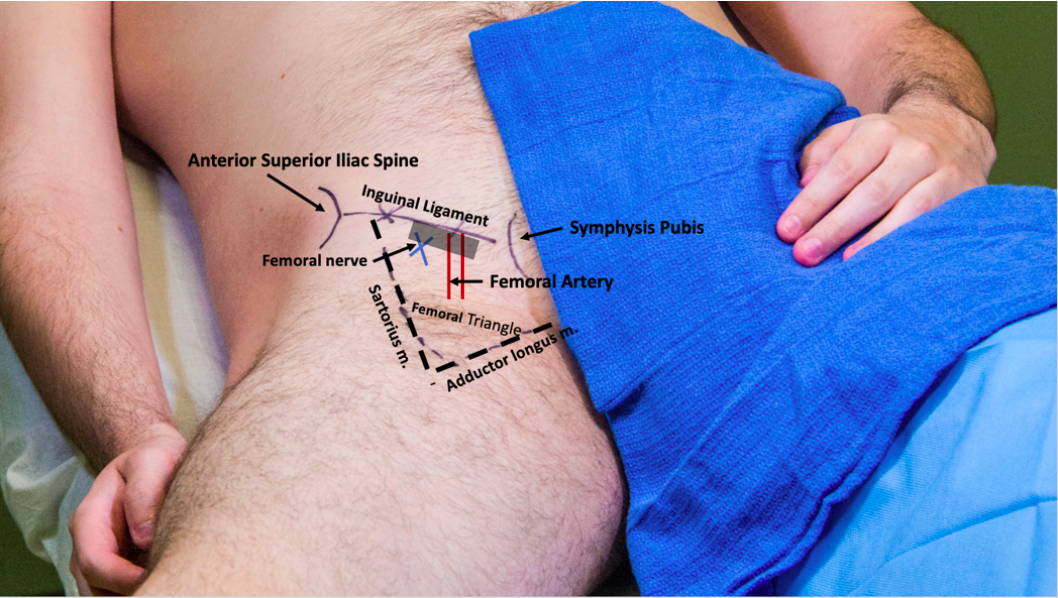
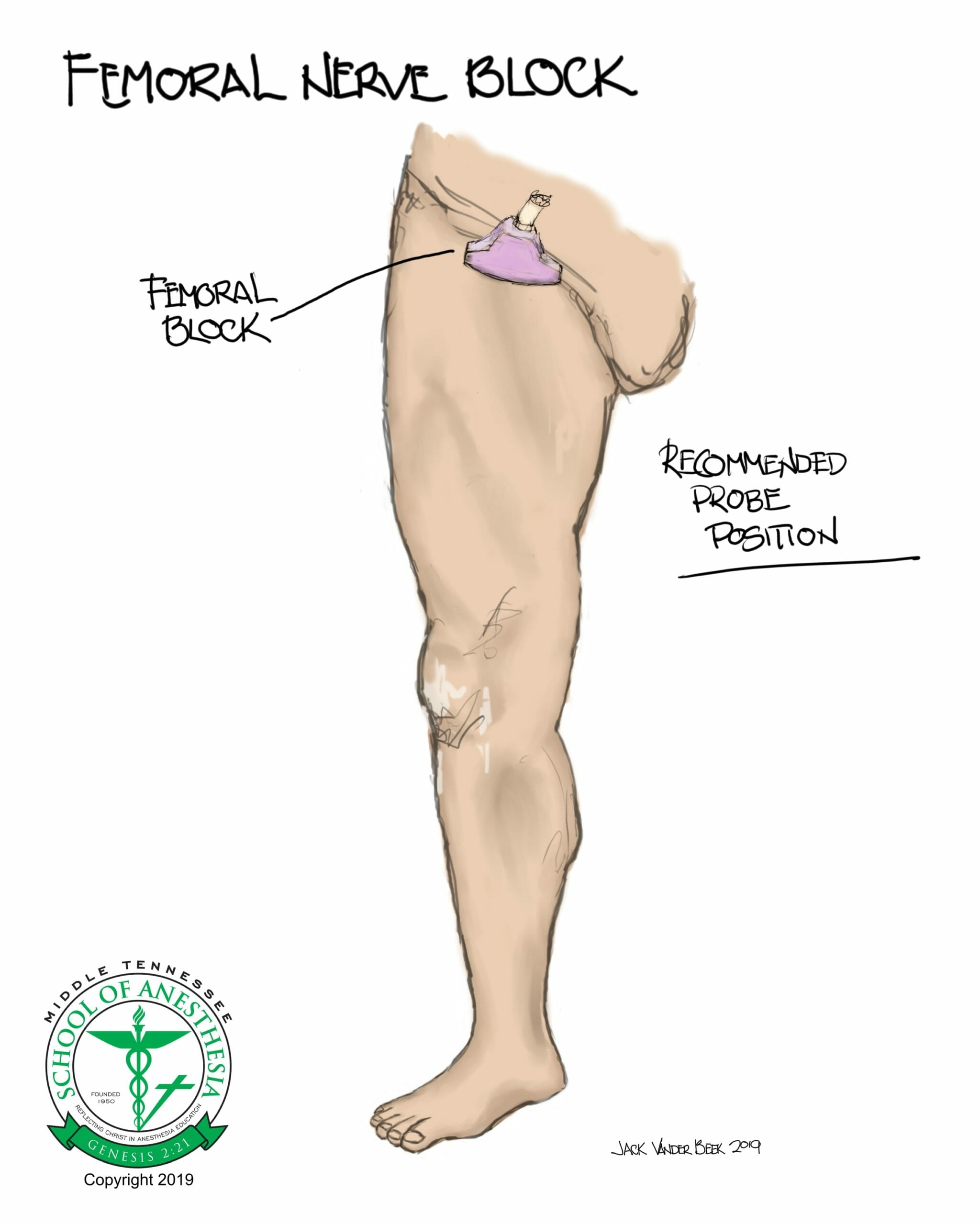
Surface Landmarks
Scanning Techniques
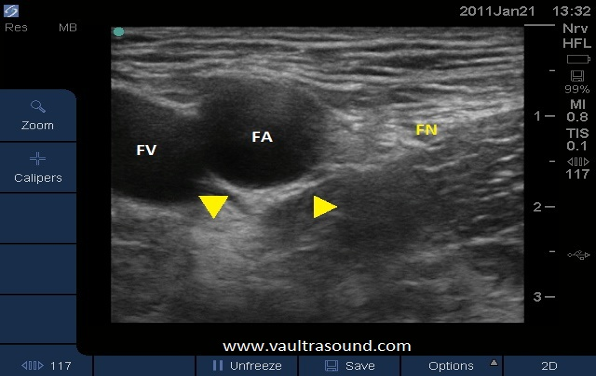
The scan for the femoral nerve begins by placing the probe lateral to the femoral artery and parallel and distal to the inguinal ligament. The probe is moved in a medial direction towards the artery until this pulsatile structure is seen in the ultrasound display. The femoral nerve lies lateral and adjacent to the femoral artery. Special attention should be given to locate the fascia iliacus layer, as the femoral nerve lies beneath this structure and has to penetrated in order to have a successful femoral nerve block.
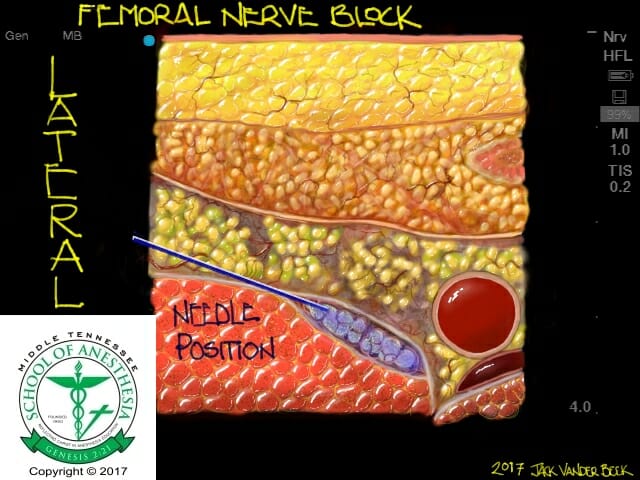
Sonoanatomy
Needle Approach
The needle is advanced using an in-plane, short axis probe approach until the needle pierces the fascia iliaca at a target location that is lateral to the femoral nerve. A distinctive “pop” will be felt when the fascia iliac is penetrated.

Nerve Stimulator Guidance
Elevation of the patella through a muscle twitch response will occur when the needle is close proximity with the femoral nerve. Adduction of the leg could indicate the incorrect stimulation of the obturator nerve, which requires needle redirection closer to the femoral nerve. Sartorius muscle stimulation (abduction of the hip) indicates anterior division stimulation and requires a slight needle redirection to a more posterior location.
Injection Technique
Local anesthetic should be injected below the fascia iliacus layer and an anechoic spread should be witnessed superiorly to the femoral nerve. Redirection and injection of local anesthetic below the femoral nerve is NOT required and could result in mechanical nerve injury from inadvertent needle-to-nerve contact.
Local Anesthetic Volume
- Femoral Nerve: 15-25 ml
Catheter Techniques
- Catheter insertion for prolonged analgesic infusions can be achieved with either an in- plane or out-of-plane approaches.
- An out-of-plane catheter insertion technique closely approximates the catheter in a longitudinal fashion along the same pathway as the femoral nerve. This technique has demonstrated reduced migration rates.
- Stimulating catheters can be placed to better approximate the catheter with the nerve and has shown to reduce infusion volumes with long-term analgesia management.
- Catheters threaded into the femoral sheath can be channeled away from the proximity of the femoral nerve. Several separate channels or compartments have been identified in this region. Use of stimulating catheters can help improve local anesthetic spread in close proximity with the femoral nerve.
- Infusions rates of analgesic strength local anesthetics can be initiated at a rate 8-10 ml/hr.
Complications
- Local anesthetic toxicity (LAST)
- Infection
- Hematoma
- Nerve injury
- Femoral nerve block with quadricep weakness is an expected result and could lead to ambulation injuries during the rehabilitation period.
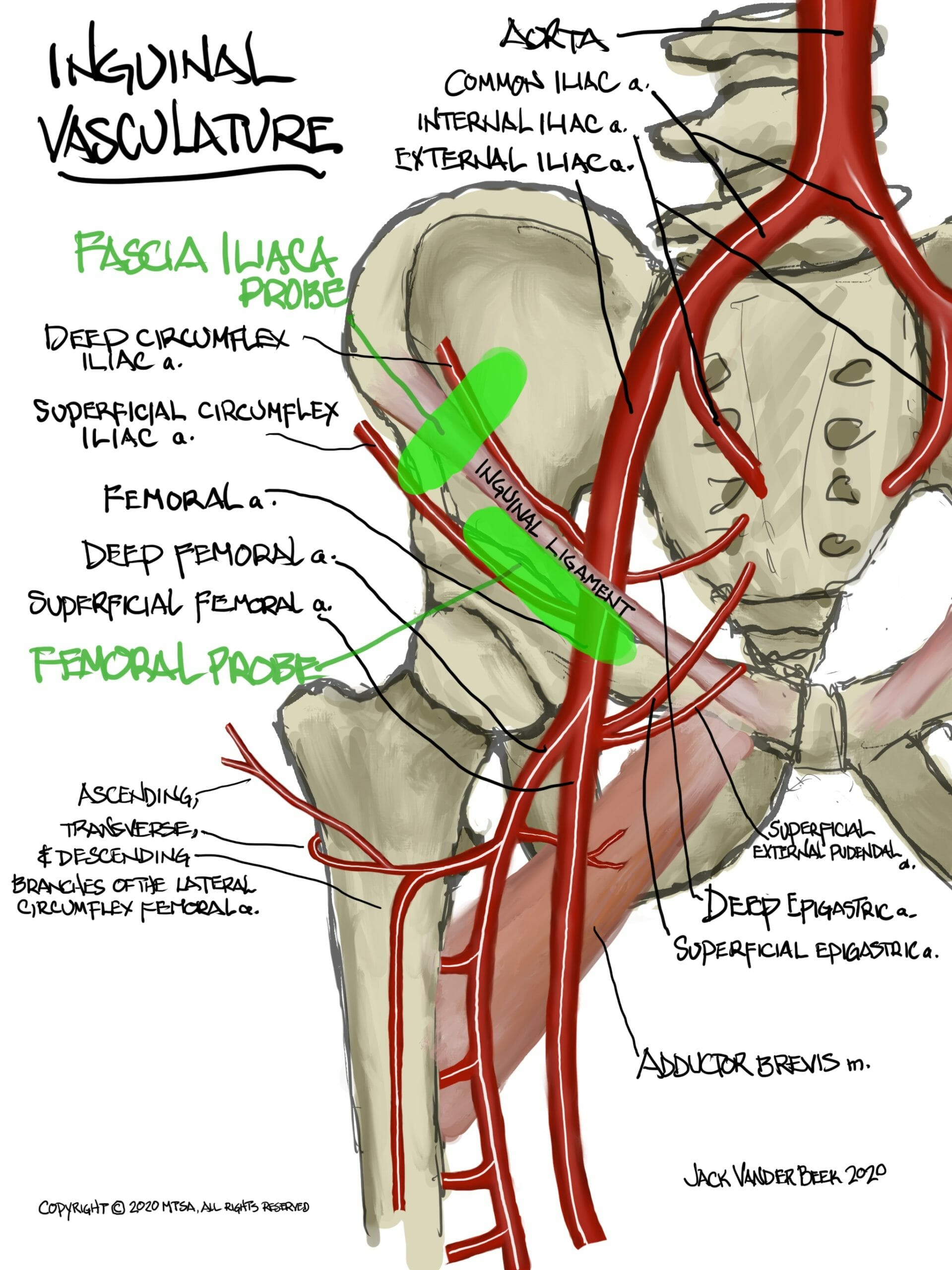
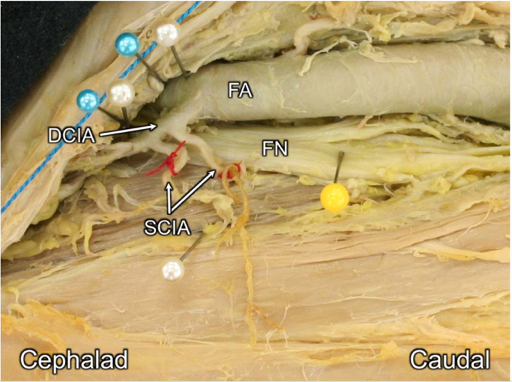
PEARLS
- On occasion, the superficial or the deep circumflex iliac artery(s) can transverse the needle path during the performance of a femoral nerve block. Application of doppler prior to performing the block can facilitate the avoidance of these structures being inadvertently penetrated with the needle tip.
Ultrasound Image of Vascular Encountered in the Needle Path of Femoral Nerve Block
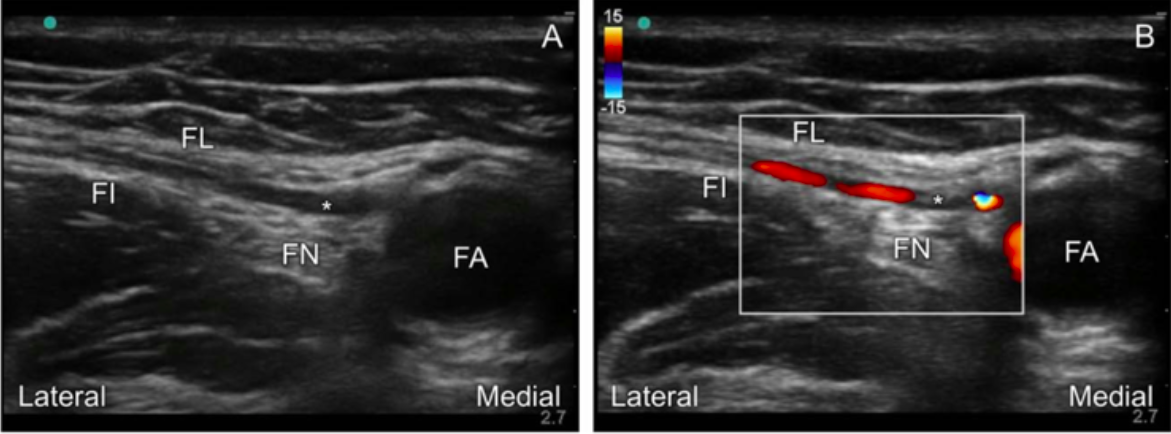
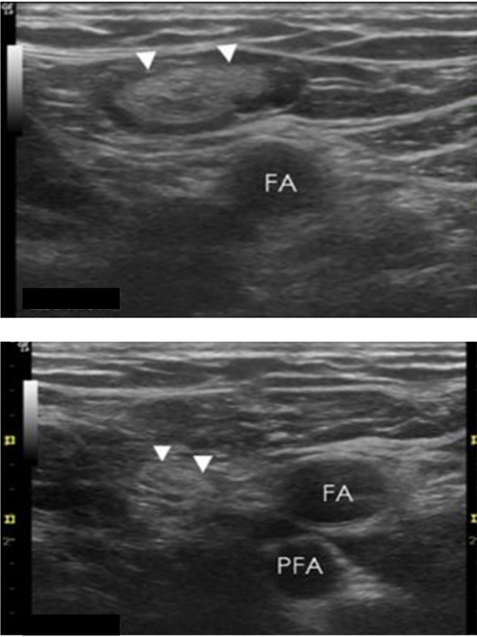
- If two pulsatile structures are encountered during scanning of the femoral block, move the probe move cephalad to avoid imaging the femoral artery where it begins branching into a deep and superficial branch at the level the femoral profunda.
- Mirrored ultrasound artifacts, hyperechoic enhancement of the femoral artery, or lymph nodes can be commonly found when scanning for the femoral nerve block. Recognition of these artifacts can be useful in avoiding placement of local anesthetic in an inappropriate location. (See examples below)
- Placement of local anesthetic beneath the fascia iliaca is critical for block success. The fascia lata layer can often be miss identified as the fascia iliaca layer on ultrasound, resulting in local anesthetic being injected above the fascia iliaca and outside the femoral perineural sheath.
References
- Hadzic, Admir. Hadzic’s textbook of regional anesthesia and acute pain management. McGraw Hill Professional, 2017.
- Dang CP, Guilley J, Dernis L, Langlois C, Lambert C, Nguyen M, Pinaud M. Is there a need for expanding the perineural space before catheter placement in continuous femoral nerve blocks. Reg Anes Pain Med. 2006;31(5):393.
- Ogami K, Murata H, Akiko S, Sato S, Saiki K, Okamota K, Manabe Y, Hara T, Tsurumoto T. Deep and superficial circumflex iliac arteries and their relationship to the ultrasound-guided femoral nerve block procedure. Clin Anat. 2017; 30:413-420.